Megaloblastic anemia
Abstract:
Vitamin B12 and folic acid are essential for DNA synthesis. If these nutrients are lacking, megaloblastic anemia can occur. Since RNA-synthesis is not affected, a developmental discrepancy between the nucleus and cytoplasm occurs, i.e. delayed nuclear maturation. This leads to both ineffective erythropoiesis (early erythropoietic death) and the emigration from the marrow of macrocytic erythrocytes with a shortened survival. Granulopoiesis and megakaryocytopoiesis are also affected, although usually to a lesser degree. Etiologies of megaloblastic anemia include deficiency of intrinsic factor in atrophic gastritis (anti-parietal cell autoantibodies and anti-intrinsic factor autoantibody = pernicious anemia) or post-gastrectomy, malabsorption as well as deficient diets which result in vitamin B12 deficiency.
Folic acid deficiency occurs with increased requirement (pregnancy, hemolysis), malabsorption and alcoholism.
Clinical picture:
The typical symptoms of anemia are present. Moreover, a painful glossitis and cheilosis can occur in a vitamin B12 deficiency. Another manifestation of vitamin B12 deficiency is subacute combined degeneration with ataxia due to demyelinization of the dorsal columns and of the pyramidal tract in the spinal cord. It may also be associated with abnormal proprioception and vibratory sensation. These neurological symptoms may occur without blood abnormalities and may, if untreated, lead to irreversible damage.
Hematology:
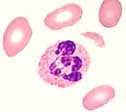 The peripheral blood film is characterized by large, often oval erythrocytes (oval macrocytes) and hypersegmented neutrophils. Leukopenia and thrombocytopenia are often present in addition to macrocytic anemia. Hyperbilirubinemia and increased LDH are signs of the intramedullary hemolysis (ineffective erythropoiesis). A definite diagnosis is established by measuring serum vitamin B12 and/or serum folic acid levels.
The peripheral blood film is characterized by large, often oval erythrocytes (oval macrocytes) and hypersegmented neutrophils. Leukopenia and thrombocytopenia are often present in addition to macrocytic anemia. Hyperbilirubinemia and increased LDH are signs of the intramedullary hemolysis (ineffective erythropoiesis). A definite diagnosis is established by measuring serum vitamin B12 and/or serum folic acid levels.
Bone marrow:
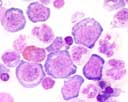 The bone marrow in megaloblastic anemia is typically hypercellular. Erythropoiesis is usually more affected. The early stages of development predominate. The discrepancy between the maturation of the nucleus and cytoplasm (cytonuclear dissociation) is characteristic. All cells are larger and demonstrate an unusually fine chromatin pattern of the nucleus. The nuclei may show karyorrhexis or are frequently found in mitosis. In granulopoiesis, large metamyelocytes and band neutrophils with enlarged nuclei are present.
The bone marrow in megaloblastic anemia is typically hypercellular. Erythropoiesis is usually more affected. The early stages of development predominate. The discrepancy between the maturation of the nucleus and cytoplasm (cytonuclear dissociation) is characteristic. All cells are larger and demonstrate an unusually fine chromatin pattern of the nucleus. The nuclei may show karyorrhexis or are frequently found in mitosis. In granulopoiesis, large metamyelocytes and band neutrophils with enlarged nuclei are present.
A bone marrow examination is not always necessary in megaloblastic anemia.
Table of Contents