������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������../../Images/malaCycle.jpg" style="border-width: 1px; border-style: solid; margin:5px 0px; line-height: 1.4em;" typeof="foaf:Image" />
Sporozoites: In the case of a bite (1) from an infected Anopheles mosquito, sporozoites reach the bloodstream of the human and from there move into the hepatic cells (2).
Schizonts: These are the final stages of the intracellular proliferation of the plasmodium. Liver schizonts , (3) which form by proliferation of the sporozoites in liver cells, are differentiated from blood schizonts (4), which result from the proliferation of merozoites in the erythrocytes.
Merozoites: With the rupture of the liver schizonts and liver cell and/or the blood schizonts and the erythrocytes, the merozoites ( 5)move into the bloodstream, where they invade other erythrocytes. They are recognizable in the microscope as ring forms.
Trophozoites: These correspond to the intra-erythrocytic stage between merozoites and schizonts (6).
Gametocytes: A part of the merozoites which originated in the erythrocytes develop in the blood to become male and female gametocytes (7). When gametocytes move into the stomach of the mosquito during feeding, the cycle is completed.
Clinical picture:
At the beginning of a malaria infection, the symptoms can be non-specific. Fevers, anemia, thrombocytopenia, splenomegaly and icterus follow later. Cerebral malaria in infections with plasmodium falciparum is most feared.
Detection of malarial parasites:
The only reliable way to diagnose malaria is to microscopically detect the parasites. The absence of plasmodium in the blood film does not exclude malaria. If malaria is suspected, the microscopic examination of the blood must be repeated until pathogens are detected or another cause for the symptoms can be found.
The best diagnostic sensitivity can be achieved with the so-called thick blood smear. In this test a drop of capillary blood or EDTA blood measuring about 15 mm in diameter is smeared onto a slide. The preparation must not be fixed and must dry for 20 minutes. It can then be stained for 20-50 more minutes with Giemsa. This leads to erythrocyte hemolysis and the freed parasites settle on the slide. As a result, the parasite density per visual field is 10-20 fold higher than that of a conventional blood film. Classification of the plasmodium is, however, not possible with the thick smear technique.

Pathogen detection is also possible in a regular blood film, made for a differential blood count. One disadvantage to this procedure compared to the thick blood smear is that for certain diagnosis, a high parasite density is necessary, which is only present in an advanced stage of illness. If the stain is processed with pH 7.2 instead of 6.8, Schüffner's stippling (plasmodium ovale, plasmodium vivax) is more easily visible. Unlike the thick smear, the regular blood film makes parasite differentiation possible.
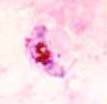
P.falciparum: The ring-like forms are small, have two chromatin bodies per ring and often occur in multiples in one erythrocyte. The gametocytes are sickle-shaped.
P.ovale and vivax: The ring-like forms are larger. Trophozoites with pseudopods occur, as well as Schüffner's stippling. Schizonts are frequent and afflicted erythrocytes appear enlarged.
The quantification of parasitemia is important for determining the success of therapy of malaria infections. Parasitemia is indicated in percent terms, therefore, a minimum of 1000 erythrocytes have to be counted.
Study the different plasmodia by looking at this schematic representations of malaria parasites.