Autoimmune hemolytic anemia (AIHA)
Abstract:
Autoimmune hemolytic anemia is an acquired disease that results from anti-erythrocytic autoantibodies, which cause red cell destruction. Warm-reactive autoantibodies of the IgG type and cold-reactive autoantibodies, which are usually type IgM, are responsible for AIHA. IgG-coated erythrocytes are removed mainly in the spleen and liver. IgM autoantibodies agglutinate the erythrocytes at low temperatures and bind complement to the erythrocytes. C3b-opsonisized erythrocytes are rapidly removed by the spleen and liver.
Clinical picture:
The warm type of autoimmune hemolytic anemia is the more frequent form. About half of the cases are idiopathic, while the other half occur secondarily in lymphoproliferative syndromes (e.g. chronic lymphocytic leukemia), infections (for example HIV), connective tissue diseases or certain medications (e.g. methyldopa). The antibodies cannot usually be identified and attack membrane antigens which occur on all erythrocytes. In severe cases, anemia symptoms exist. Splenomegaly is often present. The hemolysis leads to an increase of the non-conjugated bilirubin, which is sometimes also manifested as jaundice. The increased lactate dehydrogenase (LDH) is a good indicator of the extent of hemolysis. The direct Coombs test is positive, and the haptoglobin decreased (see parameters of hemolysis).
The cold type of autoimmune hemolytic anemia is more rare and is normally caused by IgM autoantibodies, that demonstrate an anti I-specificity in most cases. The erythrocytes agglutinate at cooler temperatures, which is why acrocyanosis, Raynaud's phenomenon and even ulcerations can occur. The symptoms are usually more marked in winter. No cause can often be found in many cases (idiopathic). However, associations are also frequently made with lymphoproliferative syndromes and infections (e.g. mycoplasma).
 Hematology:
Hematology:
Autoimmune hemolytic anemia is normally normochromic and normocytic. If the reticulocyte count is high, however, a macrocytic component also exists. In addition, anisocytosis and polychromasia are also typical. Increased erythropoiesis can be demonstrated from the reticulocyte count and even better from the red cell production index.
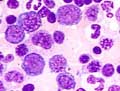 Bone marrow:
Bone marrow:
Increased erythropoiesis is found in the bone marrow.
Table of Contents