Chronic lymphocytic leukemia (CLL)
Abstract:
CLL constitutes 25% of all leukemias. It belongs to the group of lymphoproliferative syndromes. CLL almost exclusively occurs in older age patients and rarely occurs before age 40. The diagnosis is often found by chance with routine blood counts, in asymptomatic patients. CLL progresses slowly and therapy is only given once symptoms occur.
Clinical picture:
This disease remains asymptomatic for many years. Symmetrical swelling of the lymph nodes and splenomegaly are frequent. The degree of anemia and thrombocytopenia is of central prognostic importance. After years of bone marrow infiltration, normal hematopoiesis is increasingly impaired leading to worsening cytopenias, frequently resulting in serious infections. In most cases, therapy with alkylating agents usually leads to a rapid improvement in symptoms. However, therapy has no clear influence on survival. Hypogammaglobulinemia leads to increased respiratory infections. Autoimmune hemolysis occurs in around 10% of the cases.
Hematology:
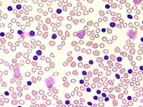 A persistent increase of small, mature, B-lymphocytes greater than 10 x 109/L accompanies CLL. The lymphocyte count can achieve values up to 150 x 109/L. Crushed lymphocytes, or smudge cells, seen in the blood film are typical for CLL. Anemia and thrombocytopenia are signs of increasing bone marrow infiltration.
A persistent increase of small, mature, B-lymphocytes greater than 10 x 109/L accompanies CLL. The lymphocyte count can achieve values up to 150 x 109/L. Crushed lymphocytes, or smudge cells, seen in the blood film are typical for CLL. Anemia and thrombocytopenia are signs of increasing bone marrow infiltration.
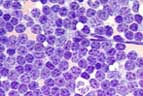 Bone marrow:
Bone marrow:
In the bone marrow an infiltration of small lymphocytes of over 40% exists. Normal hematopoiesis is more or less replaced.
Table of Contents