Acute myelocytic leukemia (AML)
Abstract:
Acute myelocytic leukemias are clonal diseases of the pluripotent hematopoietic stem cell. Genetic damages lead to abnormal precursor cells(blasts), that proliferate unchecked on one side and do not mature like the normal hematopoiesis on the other side. By the massive proliferation of blasts in the bone marrow and later in the blood, hematopoiesis is completely replaced. As consequence, on one hand side cytopenia occurs and on the other hand side symptoms such as fatigue, weight loss, fever and cachexia.
Clinical picture:
AML can appear at any age but is more frequent at median and higher age. The symptoms are characterized by failure of hematopoiesis. Pallor, fatigue and weakness are due to anemia. Bruises and petechia are due to thrombocytopenia . Neutropenia leads to infections with fever. Enlargement of liver, spleen and lymph nodes occurs in about half of the patients. Untreated, the disease is almost always lethal within few weeks to months.

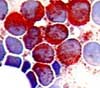
AML is mostly leukemic, i.e. there are blasts in the peripheral blood with modest to very high total leukocyte counts (occasionally >200x109/L). More rarely, the can be aleukemic. In this case, total leukocyte count can be decreased with no or only few blast in the peripheral blood. A typical example is the acute promyelocytic leukemia (APL).
Hyporegenerative, normochromic, normocytic anemia as well as thrombocytopenia and neutropenia of varying degrees are present. Myelocytic blasts can vary in size between small (a little bigger than lymphocytes) and very large (larger than promyelocytes). The cytoplasm is medium broad to broad, deep basophil to blue greyish and can be without granules, slightly granular or very granular. The shape of the nuclei is also variable from small round nuclei to large bulky, in parts lobular nuclei. The chromatin is usually very fine with one to many nucleoli. Auer rods are especially large azurophilic granules and are diagnostic for AML or RAEB-2.
Bone marrow:
The bone marrow is typically moderate to hypercellular. Sometimes, even the fatty tissue is lacking („packed marrow“). By definition, the blasts must account for more than 20% of all cells. They can reach more than 95% . Mostly, the normal hematopoiesis is completely suppressed.
Classification:
The detailed classification of acute myelocytic leukemias can be found in the information unit WHO classification. This classification is contrary to the outdated FAB-classification not only based on morphological criteria. It tries to define biological entities that differ by their natural course, prognosis or response to therapy. In order to do this, anamnestic, clinical, immunologic, cytogenetic and molecular genetic criteria are also taken into consideration. As an example, the group of therapy-related myeloid neoplasms and AML with myelodysplasia-related changes have in general a poor prognosis. Other leukemias with defined genetic lesions such as the acute promyelocytic leukemia with t(15;17), PML-RARA, the AML with t(8;21), RUNX1-RUNX1T1 or the AML with inv(16), CBFB-MYH11, show a good response to treatment with a high proportion of relapse-free survival.
Diagnosis:
When suspecting AML, the evaluation is complex and relies on the interpretation of the peripheral blood, of the bone marrow aspirate and biopsy using cytochemical staining, molecular analysis, flow cytometric immunophenotyping and cytogenetics.