Chronic lymphocytic leukemia (CLL)
Abstract:
Chronic lymphocytic leukemia constitutes 25% of all leukemias. CLL is a CD5-positive B-cell-lymphoma with shedding of corresponding lymphocytes into the peripheral blood. It belongs to the mature lymphatic neoplasms. Characteristic is a marked lymphocytosis with mainly small lymphocytes. CLL almost exclusively occurs in older age patients and rarely occurs before age 40. The diagnosis is often found by chance with routine blood counts, in asymptomatic patients. CLL progresses slowly and therapy is only given once symptoms occur.
Small cell lymphocytic lymphoma is the non-leukemic variant of CLL..
Clinical picture:
This disease remains asymptomatic for many years. Symmetrical swelling of the lymph nodes and splenomegaly are frequent. The degree of anemia and thrombocytopenia is of central prognostic importance. After years of bone marrow infiltration, normal hematopoiesis is increasingly impaired leading to worsening cytopenias, frequently resulting in serious infections. The disease cannot be cured. Therapy is based on a combination of alkylating agents, purine analogues and anti-CD20- antibodies. Recently, therapy with oral B-cell-receptor-signal-way-inhibitors and bcl-2-inhibitors showed promising improvements of response. Usually, a rapid response to drug therapy can be observed with resolving the lymphocytosis, disappearance of cytopenia and improvement in symptoms that can last for many years. However, therapy has no clear influence on survival. Only allogenic stem cell transplantation in selected young patients can lead to lasting remissions.
Hypogammaglobulinemia leads to increased respiratory infections. Autoimmune hemolysis occurs in around 10% of the cases.
Hematology:
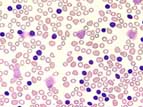
A persistent increase of small, mature, B-lymphocytes greater than 10 x 109/L accompanies CLL. The lymphocyte count can achieve values up to 150 x 109/L. Crushed lymphocytes, or smudge cells, seen in the blood film are typical for CLL. Anemia and thrombocytopenia are signs of increasing bone marrow infiltration.
Bone marrow:
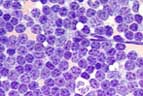
In the bone marrow an infiltration of small lymphocytes of over 40% exists. Normal hematopoiesis is more or less replaced.
Since diagnosis is usually based on flow cytometric immunophenotyping in the peripheral blood, a bone marrow aspiration is not necessary. However, bone marrow examination is usually performed before the beginning of therapy.
Diagnosis:
According to the WHO 2016 classification, the diagnosis of CLL can be established based on > 5 x 109/L monoclonal B-cells and the typical CLL-immunophenotype. The immunophenotype of CLL is very characteristic and, in almost all cases, allows for clear differentiation from other B-cell lymphomas with elevated lymphocyte counts in the peripheral blood. CLL-cells are positive for CD19, CD5 and CD43. In contrast to "wild type" B-cells and many other B-cell-lymphomas, CD20, CD22, CD79b, CD81 and superficial immunoglobulins are diminished or negative. Typically, FMC7 is completely lacking. The strong expression of CD200 allows for the differentiation from CD5-positive, but usually CD200-negative mantle cell lymphoma.