Iron deficiency anemia
Abstract:
Iron deficiency anemia is the most frequent form of anemia worldwide. In developing countries, it is normally caused by malnutrition or parasitosis. In western countries, the most frequent cause is a chronic loss of blood (menometrorrhagia, ulcer disease, carcinomas of the gastrointestinal tract, hematuria).
Clinical picture:
The typical symptoms of anemia exist. Moreover, iron deficiency can lead to nail abnormalities, angular cheilosis (perlèche), glossitis and dysphagia (Plummer-Vinson syndrome).
Hematology:
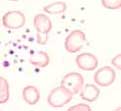
Iron deficiency anemia is typically hypochromic and microcytic (MCV and MCH decreased, MCHC normal or decreased). In the blood film, microcytosis and hypochromia are found, in addition to a distinct anisocytosis and poikilocytosis. Thrombocytosis is also not uncommon. A decreased serum iron, decreased transferrin saturation, and decreased serum ferritin confirm the diagnosis of iron deficiency anemia.
Seven to ten days after starting iron therapy, an increase of reticulocytes can be observed. Since reticulocytes have a higher volume, MCV increases. This causes in the initial phase an discrepancy between MCV and MCH values. In severe iron deficiency anemia, MCHC is also decreased. An early sign of iron deficiency ls an increased RDW.
Bone marrow:
The examination of the bone marrow is not necessary for the diagnosis of iron deficiency anemia. The demonstration of lacking storage iron by the Prussian blue staining is indicative for iron deficiency. However, sensitivity and specificity of this examination are low.