Acute lymphoblastic leukemia (ALL)
Abstract:
ALL is typical childhood leukemia that most often occurs between the ages of 2 and 5. A second peak can be observed in higher age. Malignant lymphocytes replace the blood-forming bone marrow and infiltrate the lymph nodes, spleen, liver and other organs. Most children do not survive very long without therapy. However, many patients go into remission after undergoing different forms of cytostatic therapy. Patients with childhood ALL have great potential to be cured.
Clinical picture:
The disease begins abruptly and rapidly increases in severity. The symptoms result from infiltration of the bone marrow leading to neutropenia, anemia and thrombocytopenia. Weakness, pallor, fevers and bleeding occur. Additional symptoms include irritability, loss of weight and appetite, as well as aching of the joints. Headaches and vomiting can be signs of involvement of the central nervous system. Enlargement of the spleen, liver and lymph nodes is usually present. Mostly in T-lymphoblastic leukemia, a big mediastinal tumor (bulk) is found.
Hematology:
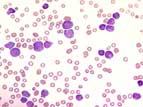
In about 50% of cases, leukocytosis with distinct neutropenia exists. The blasts are usually small and have high nuclear-cytoplasmatic ratio, blurred chromatin, and indistinct nucleoli. Normochromic, normocytic anemia is seen. Staining with peroxidase and esterase is negative. A cytological distinction between acute B- and T-lymphoblastic leukemia is not possible. Normochromic normocytic anemia can be very pronounced.
Bone marrow:
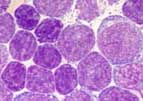
The bone marrow is normally hypercellular with dense infiltration by small blasts without granules. The lymphoblasts stain negatively for peroxidase and esterase.
Classification:
According to the WHO-classification, acute lymphoblastic leukemias are called lymphatic precursor cell-neoplasms based on the postulated lineage from immature lymphatic precursor cells. This is to emphasize the distinction form mature cell lymphatic neoplasms (lymphomas). Acute leukemias can be of B-lineage (B-ALL) as well as of T-lineage (T-ALL). Similar as in acute myelocytic leukemias, acute B-lymphoblastic leukemias with recurrent genetic abnormalities and characteristic biological behavior are listed separately in the WHO classification. While the acute lymphoblastic leukemias can proceed "leukemically", lymphoblastic processes can be confined to lymph nodes or extramedullary tissues. These cases are called acute lymphoblastic lymphomas. Their course of disease is not different from the course of ALL. The FAB-classification (F=French, A=American, B=British) is no longer used.
Diagnosis:
In the classification of ALL, flow cytometric immunophenotyping is of outstanding importance since it provides a fast attribution of lineage and reliable distinction from AML. Cytogenetical and molecular examinations are also important for the classification and prognostic risk estimate.