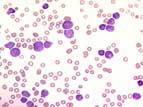
 In about 50% of cases, leukocytosis with distinct neutropenia exists. The blasts are usually small and have high nuclear-cytoplasmatic ratio, blurred chromatin, and indistinct nucleoli. Normochromic, normocytic anemia is seen.
In about 50% of cases, leukocytosis with distinct neutropenia exists. The blasts are usually small and have high nuclear-cytoplasmatic ratio, blurred chromatin, and indistinct nucleoli. Normochromic, normocytic anemia is seen.Abstract:
ALL is typical childhood leukemia that most often occurs between the ages of 2 and 5. Malignant lymphocytes replace the blood-forming bone marrow and infiltrate the lymph nodes, spleen, liver and other organs. Most children do not survive very long without therapy. However, many patients go into remission after undergoing different forms of cytostatic therapy. Patients with childhood ALL have great potential to be cured.
Clinical picture:
The disease begins abruptly and rapidly increases in severity. The symptoms result from infiltration of the bone marrow leading to neutropenia, anemia and thombocytopenia. Weakness, pallor, fevers and bleeding occur. Additional symptoms include irritability, loss of weight and appetite, as well as aching of the joints. Headaches and vomiting can be signs of involvement of the central nervous system. Enlargement of the spleen, liver and lymph nodes is usually present.
Hematology:
In about 50% of cases, leukocytosis with distinct neutropenia exists. The blasts are usually small and have high nuclear-cytoplasmatic ratio, blurred chromatin, and indistinct nucleoli. Normochromic, normocytic anemia is seen.
Bone marrow:
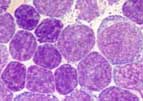 The bone marrow is normally hypercellular with an infiltration by blasts of over 30%. The lymphoblasts stain negatively for peroxidase and Sudan-black but are terminal deoxynucleotidyl transferase positive.
The bone marrow is normally hypercellular with an infiltration by blasts of over 30%. The lymphoblasts stain negatively for peroxidase and Sudan-black but are terminal deoxynucleotidyl transferase positive.
Classification:
Like the acute myelocytic leukemias the acute lymphocytic leukemias are classified based on their morphology by FAB (F=French, A=American, B=British). There are 3 types:
L1: Most frequent form found in children. The morphology of the blasts is uniform and largely corresponds to that described above.
L2: Most frequent form found in adults. The morphology of the blasts can vary widely form case to case and even within a case. The cytoplasm is distinct and occasionally contains peroxidase-negative granules.
L3: Rarest form, also call the Burkitt type, with .
Immunophenotyping has played an important role in classifying ALL. Cytogenetics and increasingly molecular diagnostic test are also valuable.