Acute myelocytic leukemia (AML):
Abstract:
AML most often occurs in adults. Its frequency increases in adults over age 50. Without therapy most patients only survive for a few months. By implementing different myelosuppressive chemotherapies, high rates of remission can be achieved.
Clinical picture:
The symptoms are characterized by failure of hematopoiesis. Pallor, fatigue and weakness are due to anemia. Bruises and petechiae are due to thrombocytopenia. Neutropenia leads to infections and fever. Enlargement of the liver, spleen and lymph nodes occurs in about half of the patients.
Hematology:
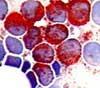
 Normochromic, normocytic anemia always exists. The platelets are usually moderately decreased. The leukocyte count can vary between <1x109/L and >100x109/L. The presence of blasts in peripheral blood is diagnostic. Azurophilic granules indicate the presence of a myelocytic leukemia. The presence of Auer rods is pathognomonic for AML.
Normochromic, normocytic anemia always exists. The platelets are usually moderately decreased. The leukocyte count can vary between <1x109/L and >100x109/L. The presence of blasts in peripheral blood is diagnostic. Azurophilic granules indicate the presence of a myelocytic leukemia. The presence of Auer rods is pathognomonic for AML.
Bone marrow:
 The bone marrow is typically hypercellular. Special staining with peroxidase is used to determine whether blasts are myeloid in origin.
The bone marrow is typically hypercellular. Special staining with peroxidase is used to determine whether blasts are myeloid in origin.
Classification:
Like the acute lymphatic leukemias the acute myelocytic leukemias are classified by FAB (F=French, A=American, B=British) based on their morphology. There are 8 types:
M0 = undifferentiated myelocytic leukemia: Less than 3% of the blasts are peroxidase-positive.
M1 = myelocytic leukemia without maturation: The blasts are slightly differentiated, have minimal cytoplasm and fine nuclear chromatin with clear nucleoli. In bone marrow, at least 3% of the blasts must be peroxidase-positive.
M2 = myelocytic leukemia with maturation: The blasts are large with ample cytoplasm with azurophilic granules. Auer rods are frequent. Around 20% of the AML M2 patients have a translocation (8; 21).
M3 = promyelocytic leukemia: The blasts are very rich in azurophilic granules. Numerous Auer rods are typical. With cell death, the released enzymes from these granules can lead to the appearance of disseminated intravascular coagulation. This is associated with a high mortality rate. This complication has become increasingly rare with the use of all trans retenoic acid. This drug (combined with chemotherapy) has increased the survival rates of patients with M3 dramatically.
M4 = myelomonocytic leukemia: AML with myeloid and monocytic maturation. Gingival hyperplasia occurs in 10% of the patients.
M5 = monocytic-leukemia: Infiltration of the skin, mucous membranes, lungs, colon, meninges, lymph nodes, and larynx are very frequent. Over 80% of the blasts in the bone marrow are monocytic.
M6 = erythroleukemia: Rare. Over 50% of the nucleated bone marrow cells belong to the red line and over 30% of the remaining cells must be blasts of the M1 or M2 type.
M7 = megakaryoblastic leukemia: Rare. Usually refractory to therapy.
Immunphenotypic, cytogenetic, and molecular (e.g., proof of the fusion transcripts with RT-PCR) diagnostic test are playing an increasingly important role in the classification of leukemias today.
Table of Contents